Shapes of Experience
Neuroscience, Developmental Psychology,
and Somatic Character Formation
Marianne Bentzen, Denmark33
Marianne Bentzen is a co-founder of Bodynamic Analysis and the Bodynamic Institute in Copenhagen, which have gained an international reputation for their specific and differentiated concepts on Somatic Developmental Psychology. She comes from a background as a psycho-motor therapist, with further training in the tradition of Biosynthesis (Boadella), Somatic Experiencing (Levine), Systems-Centered Training (Agazarian), meditation, and interpersonal neurobiology. After retiring from her position in the faculty of the Bodynamic Institute, where she also served as training director for thirteen years, she has co-founded, with psychologist Susan Hart, a developmental neuroaffective approach to psychotherapy. She currently has a private practice and conducts trainings independently in Scandinavia and Europe.
Bentzen has presented her work at numerous European universities and in psychiatric hospitals, has published a series of scientific papers, has written several chapters in books, and has co-authored at least one book in Danish. She is a member of the psychotherapy association of Denmark, and was the chairperson of the ethics committee of the European Association for Body Psychotherapy for several years.
I am not saying that the mind is in the body. I am saying that the body contributes more than life support and modulatory effects to the brain. It contributes a content that is part and parcel of the working mind. —Damasio (1994, p. 226)
This chapter compares findings in developmental neuroscience and infant research, from children from birth to two years old, with five basic somatic character structures derived from the slightly varied descriptions of development in three different somatic character systems: Bioenergetics, Hakomi, and Bodynamics. These comparisons show: (1) a strong correspondence between neuroaffective development, posture, and behavior of misregulated children, and the somatic character structures for which that age is considered a formative stage; and (2) that the developmental stages, traditionally described as oral, anal, and oedipal, are—contrary to current characterological thinking—usually activated before the child is two years old.34
Introduction
Like traditional character-analytical theories, most theories about somatic character rest on Developmental Psychology. They posit that, with the formation of emotional and psychological patterns, there is a formation of motor habits and “energy” patterns in the body that develop according to key interactive patterns throughout childhood. Body Psychotherapists assume that central parts of the personal narrative are accessible only in the inner sensory field, and that they are existentially grounded in the person’s motor patterns and habits.
A widespread misunderstanding about somatic character theory is the belief that it claims that body structure creates personality. The true theoretical foundation of somatic character development is that experience shapes the body, as well as the psyche, in coherent and characteristic ways. Put differently, all experience has somatic components that shape neuroaffective habits, whereas experience and affect both shape neuromotor habits.
In Somatic Psychotherapy, the body is considered to be an essential part of the story of the psyche, but definitely not the whole story. In reading the somatic character structure in the adult or in the older child, the therapist is reading stages of affect and affect regulation, visible in the motor system, and is “reasoning backward” from there. If a person is showing postures, movements, and gestures typical of a certain developmental age and interaction, the therapist assumes that corresponding states of neurological activity, self-representations, and affect (psycho-social character) are present to some degree or other (Bernhardt, Bentzen, and Isaacs, 1996). As in the usual psychodynamic approach, the therapist relies on the verbal narrative of the client to flesh out the story of the postural habits he is seeing. Reich said that character is frozen history. Perry and colleagues (1995) state, “Experience can change the mature brain—but experience during the critical periods of early childhood organizes brain systems!” (The original was in capitals and italics!)
Somatic character theories view a specific character structure as shaped both at the age at which a certain neurological and interactional maturity develops, and also by those earlier and later experiences—including current lifestyle—that resonate with theme and level of processing and interaction inherent to that maturity. Any individual with normal levels of brain function will thus show elements of all the character structures.
Formative Factors in Character Formation
In recent decades of developmental research and brain research, there has been a great deal of scientific inquiry into the formative dynamics of the personality. Geneticists and developmental researchers alike agree that virtually all psychological and physiological traits develop out of an intimate interplay between genetic predisposition and environmental influence (Perry, 2002; Ridley, 2003; Rutter, 2006; Cuhna and Heckman, 2010; Tabery and Griffiths, 2010). Inborn temperament can be tested in early infancy, shows stability (Chess and Thomas, 1996; Kagan, Snidman, Kahn, and Towsley, 2007), and is shaped by the quality and availability of the intersubjective field, that sense of shared presence between infant and caregiver (Thelen and Smith, 1994; Aitken and Trevarthen, 1997; Beebe and Lachmann, 2002; Stern, 1995, 2004; Gerhardt, 2004; Hart, 2011). We need the loving attention of another to become a self.
Three mental states (Stern, 1995, 2004) are considered central to good intersubjective attunement: shared attention, shared intention, and the ability to participate in the affective states of another. Attunement is a delicate process consisting of thousands of daily, tiny, interlocking dance movements, in which, in the healthy parent-child relationship, the synchrony of misattunements occurs dozens or hundreds of times each day (Tronick and Gianino, 1986; Tronick and Weinberg, 1997). However, misattunements on average last only two seconds, because both the parent and the child have a biological desire to reattune. Research indicates that it is the repair through somatic resynchronization rather than the absence of misattunement that develops basic trust and healthy maturation (Trevarthen, 1979, 1990, 1993a, 1993b). Pervasive or unrepaired misattunements may be caused simply by lack of sufficient attunement capacity in the caregiver, perhaps caused by underlying stressors, as well as by specific traumatic events. Character defenses develop from ingrained habits, because infants, for better or worse, easily identify and prefer the interaction patterns they are used to (Sander, 1977, 1983, 1987, 1988; Bentzen, Jarlnaes, and Levine, 2004; Hart, 2011). Fortunately, the dance of microattunement through somatic mirroring allows the child to directly absorb and identify positive inner states of the caregiver, as well as negative (Stern, 1995).
The neural mirror systems are a complex brain network of neurons that allow humans to experience the intention movements and feeling states of others as their own. Mirror-system activation is essential to empathic capacity, and is activated by seeing, hearing, or even reading about the movements and feelings of others, or even by experiencing the touch of others (Gallese, Fadiga, Fogassi, and Rizzolatti, 1996; Gallese and Goldman, 1998; Gallese, 2001; Keysers, 2011). Infants are born with a rudimentary capacity to mirror, but it can fail to develop if it is not engaged by the mirroring of the caregiver (Perry and Slavavitz, 2007). In children as well as adults, mirror activity in the brain is weakened or deactivated by stress. Mirroring is also affected by power relationships (Hogeveen, Inzlicht, and Obhi, 2014). In interactions with attention to one person having power over another, the empowered person responds with reduced empathy and mirror activity in the brain, while the weaker person responds with increased mirror activity.
Specific traumatic events are perhaps the most commonly considered reason for personality problems. However, according to developmental research, it is primarily the millions of microinteractions, beginning before birth and continuing throughout life, that create the very experience of our being in the world; and the thousands of microattunements with a caring therapist that can later improve one’s self-sense in therapy (Stern, 2004).
Finally, different stages of development offer different themes and challenges to the child and the parent (Hart, 2011; Hart and Bentzen, 2012). The parent-child microinteractions during these different stages will shape somatic character through the interaction and psycho-motor skills that the child is developing at the time. Traditionally, the character structures are seen to develop during the first six years or so of life. However, while writing this chapter, I found to my considerable surprise that in terms of neuroaffective development, the core issues of all five character structures are activated during the first twenty-four months of life.
Three Systems of Somatic Developmental Character Structure
There are many different systems of somatic character: Reich (1949) began to work with the body in the 1930s, and developed the first systematic method of psychodynamic somatic character structure. All later schools have built on, or been influenced by, his concepts. In the following, I will use just three systems that are organized primarily from a developmental understanding, and that are also currently taught in trainings in Europe and North America. All three systems are still refining and changing their theories (and there are, of course, many more other Body Psychotherapeutic modalities, also in processes of develoment and change):
• Bioenergetic Analysis (henceforth called Bioenergetics) is directly descended from Reich’s work. Lowen’s first popular book about character, The Language of the Body, was published in 1958. Most other somatic character systems have been strongly influenced by this system, and (for the reader from a nonsomatic background) the relationship to traditional psychoanalytic character structure is fairly obvious. Over the intervening years, however, this system has abandoned psycho-sexual charge as the central concept and has embraced attachment theory, with flow and muscular blocking seen as a response to developmental thwarting.
• Hakomi was developed by Kurtz and his staff in the mid-1970s. It introduces the idea that character traits may be seen as “overdeveloped” skills, as well as traumatic regressions. It focuses on development as the learning processes of a self-organizing body-mind system, which requires certain healthy experiences to mature optimally. Character formation may then be understood as constructive attempts to cope with unhealthy formative interactions. Hakomi thus emphasizes more positive aspects of character.
• Bodynamic Analysis (henceforth called Bodynamics) originally developed out of a northern European tradition of psycho-motor developmental awareness work. During the 1980s, Marcher (Marcher and Fich, 2010) and her colleagues combined psycho-motor development with Bioenergetic character theory and developed a model based on motor and psychological child development, and a corresponding theory of specific muscle activation. “Mutual connection” is seen as the basic drive, rather than sexuality. The response of the environment to this basic drive determines whether healthy or unhealthy character develops.
There is a great deal of overlap between these three character models, and each also has concepts that are unique to themselves. Because this chapter functions as a brief introduction to somatic character, the main focus will be on areas of general agreement and some basic body concepts, rather than on details and differences between the systems. Unfortunately, this means that I will not devote any space to the healthy character, which is a strong focus in both Hakomi and Bodynamics. I will outline five structures described by all three systems:
I. Schizoid (hysteric)
II. Oral
III. Psychopathic
IV. Masochistic
V. Rigid (phallic and hysteric)
Although there is widespread dissatisfaction with these pathological labels, I will use them in this chapter because there are no other universally known “tags” for these somatic character structure types. All three systems present two structures at some or all character levels, such as early and late, or compensated and oral. Bodynamics, inspired by the earlier work of Johnsen (1976) on developmental resources, defenses, and resignation in the body, has two positions at each developmental stage: an early, more resigned, and posturally collapsed one, and a late, more controlled, and posturally tense one. However, all three systems use the general postural concepts of collapse and flaccidity as well as the concepts of muscular tension and character-armoring.
In this chapter, I will outline the following points for each of the five character structures: core elements of neuroaffective development and formative age, clinical descriptions and studies of children, and somatic character structures. Because the formative stages are not mutually exclusive, most people have a mixture of several character structures, though one or two often predominate.
I. Prenatal and Neonatal Development: The Autonomic Nervous System, Early Infant Contact Disturbances, and Schizoid-Hysteric Traits
Stephen Porges (1997) describes three phylogenetic stages of neural development in the autonomic nervous system and three corresponding levels of emotive and interactive behaviors. The autonomic nervous system is the part of the brain that matures first. The first two aspects of the autonomic nervous system are active at birth, and the third matures during the first six weeks after birth.
The first stage is the primitive, “unmyelinated vagal parasympathetic” system, which activates digestion and responds to novelty or threat with a reduction of metabolic output and immobilization (freezing). The second stage is the “spinal sympathetic” nervous system, which can increase metabolic output and inhibit the action of the primitive vagal system on the intestine, allowing “fight-or- flight” behaviors to emerge. The third stage is the “myelinated vagal parasympathetic” system, uniquely mammalian, which can regulate metabolism to allow fine-tuned engagement and disengagement with the surroundings. It controls facial expressions, sucking, swallowing, breathing, and vocalization. It also inhibits the sympathetic action on the heart, supporting calm behavior and pleasurable interaction.
The myelinated, social vagal system is active under conditions of normal interaction—for instance, when the baby smiles, gurgles, and makes different noises to invite food, sleep, or play. When the child is stressed, this organization gives way to the phylogenetically earlier “fight-or- flight” system. In the infant, this first means crying, and increased startle and gripping reflexes. With more intense activation, the infant screams while flailing and twisting in an increasingly disorganized manner. Finally, if there are no outlets for fight-or- flight responses, the most primitive system and the dissociative parasympathetic coping strategy become dominant: the infant withdraws, becomes passive and quiet or immobile, and shows little or no interest in contact or food.
According to Perry and colleagues (1995), the infant has two separate reaction patterns to severe stress. Perry’s descriptions correspond to Porges’s levels of activation. The first is a sympathetic arousal state, and the second is a parasympathetic dissociative state. When the infant is frightened, his heart rate and breathing increase, his blood pressure goes up, he becomes alert, and he cries. This is essentially the “fight-or- flight” response, Porges’s second phylogenetic stage of arousal. If the arousal state of the infant is not regulated, after a while he will dissociate, withdraw from external stimuli, and become extremely passive. The intense sympathetic activation is still present, but the parasympathetic inhibition overrides it. This is the action of the first phylogenetic stage of the polyvagal system. The infant is in a state of highly activated, frightened helplessness and resignation.
Brodén (2000), director of a treatment facility for disturbed infants in Sweden, describes the traits and attachment styles of infants with ongoing unregulated stress. Following the attachment research of Ainsworth and others, she describes children in three states: “overpassive,” “overactive,” and “stable.” Brodén states that the typical “overpassive” infant in her practice (corresponding to the parasympathetic, dissociative state and the schizoid structure) does not fuss, rarely invites contact, and seems content when left to his own devices. He is disinterested in food and pleasurable activities, but likes to spend time alone in bed. He is slow to engage, and rarely smiles. Even when staff members pick up this child for a cuddle, they usually put him down again quickly because he has no “molding behavior.” He doesn’t cuddle up to the body of the adult, and this makes him seem to reject the physical contact. He does not have the spontaneous somatic responses that make contact rewarding for others, so they often disengage after attempting a few times to elicit some form of welcome. Brodén emphasizes that she is describing contact-disturbed infants, and not autistic ones.
The “stable” children, in Brodén’s practice, are managing conditions of insufficient nurturing very well. Their biological functions and rhythms are simple and stable; they are easy to feed and get to sleep; and they adapt well to changes. They are described as actively “helping” their mothers with their overexpressive signals, frequent smiles, and generally positive response. Deprived of sufficient maternal response, they readily turn to others and greedily absorb contact and nurture. The motor patterns of these infants are staccato and uncoordinated. Deprived of maternal holding, Brodén reasons, they “hold” themselves with strong tensions in their back, shoulders, and neck. The staff has nicknamed them “swan-neck children” because of their long necks and tendency to hold the head stiffly. These “stable” children have trouble relaxing into holding and contact, and instead seem to stay “on alert” and to take an unreasonable amount of responsibility for the contact, particularly for eye contact. In terms of physiological activation, these infants show a fairly high level of sympathetic arousal, but still organized in contact strategies.
Brodén’s “overactive” infants have extreme and diffuse movement patterns, and may even seem spastic. Their facial expressions are worried and guarded. They actively resist body contact and eye contact, and their general activity level is very high and avoidant. They seem generally unsatisfied, and often go into incomprehensible states of crying and screaming. They are easily frustrated and upset, and difficult to calm. It is difficult for them to wait for food, and meals are like battlegrounds. When fed, they are often so upset that they have trouble settling into eating, and then quickly tire. Often they gulp their food and then throw up after eating. The infants’ biological rhythms are very irregular, and they are easily disturbed and upset. These infants live at the physiological level of disorganized sympathetic activation and fight-or- flight response.
Bioenergetics describes the developmental stages as having a “hierarchy of needs,” not unlike Maslow’s self-actualization pyramid. The basic need during intrauterine and early postnatal existence is the “right to exist”—which is internalized through being welcomed (Lowen, 1958; MacIntyre and Mullins, 1976; Ingen-Housz, 2003). Because the infant is completely dependent on parental figures for emotional as well as physical nurture, other schools emphasize that this right has meaning only when described as a “right to exist” and “to belong with someone.” When this right is threatened, schizoid or hysteric character elements result. Both respond to a “threat of annihilation”; but, whereas the schizoid structure emerges from ongoing hostility, coldness, or abandonment, the hysteric structure is generally understood as an adaptation to sudden, less constant, traumatic events. These distinctions correspond well to Porges’s and Perry’s assertions that the infant first reacts to stress with sympathetic fight-or- flight arousal, and withdraws into parasympathetic dissociation only when the threat is perceived as being more constant.
The prenatal and neonatal infant has no sense of a separate self, and is completely dependent on his caregiver for basic modulation of arousal. If he is frequently abandoned, or treated with hostility, he habituates to a constant level of fear and distress as his “normal” resting state. This is thought to be the most common formative dynamic of the schizoid character pattern. Isolation impacts the emerging self-regulation, and if the infant’s experience is not offset, the later formation of internalized objects of self and others will be hostile and depersonalized. Adults with schizoid traits describe their inner experience of their self as alien, disconnected, fragmented, and deadened. The person is identified primarily with the mind and often distrusts and dislikes the body and its unruly feelings. The social world and other people are felt to be alien, stressful, or innately hostile. As Lake (1966) puts it, “Saying good-bye is like getting a new lease on life.” If this person suddenly gets in touch with excitement and feelings, he may not be able to regulate them. These states then become synonymous with intolerable levels of arousal, terror, rage, destruction, and/ or pain. Under extreme stress, he may dissociate further into flares of rage or terror.
The schizoid posture is characterized by deep holding patterns in the core of the body, and a habituated parasympathetic dissociative activation that leaves the skin and the extremities cold. Movements are often stiff and clumsy, and there is little spontaneous movement. Even when he is trained in athletics or dance, his movements are outer-directed (which corresponds to later cortical control patterns) rather than inner-directed (corresponding to early neuromotor integration). His breathing is shallow, and the general physical impression is of a person who has withdrawn as far as possible from aliveness. Like Brodén’s “overpassive” infant, the schizoid structure does not know how to shape himself to touch and physical contact, and his body seems unresponsive to closeness. He often avoids mutual eye contact. Even when he does meet the eyes of another, his gaze seems unfocused, and the other has no feeling of an emotional or contactful meeting.
Reich viewed the schizoid character structure as having a primary blocking around the eyes and in the suboccipital orienting muscles of the neck. Their body is characterized by deep, “frozen” holding patterns in and around the joints, twists and significant differences of organization between their right and left side, as well as between different parts of the body. The description of this somatic pattern has elements of the disorganized flailing of the infant in severe sympathetic distress frozen in a matrix of dissociated primitive parasympathetic inhibition. Often the basic autonomic rhythms are in disarray: sleep patterns are fragile, digestion may be too rapid, the person is hypersensitive or numb to sensations and external stimuli, and a complaint of constant loose stools or incontinence is often heard.
Schizoid Somatic Pattern
The schizoid structure is shaped by threat of annihilation. (Bioenergetics)
Formative age: second trimester to three months (Bodynamics). Also called the “tactile” or “ocular” stage of development in other systems. This infant (Figure 27.1) was born five weeks early, and shows some very early neurosomatic organization, governed by the unmyelinated parasympathetic vagus. He has some muscle tone and beginning reflexes, which make him flex his legs and fingers and turn his head, tilting it a bit backward.
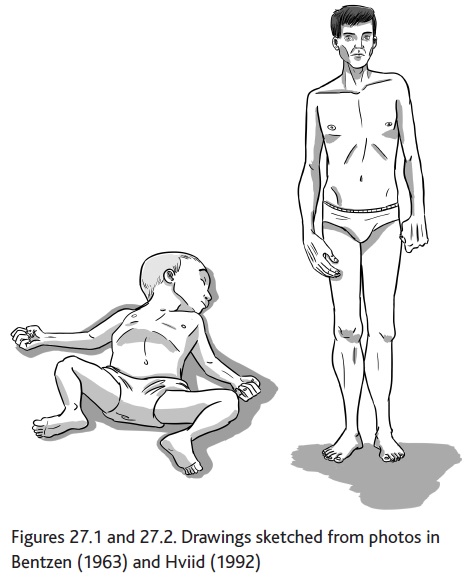
This man has been asked to stand straight (Figure 27.2). His posture shows the asymmetry and twists of the schizoid pattern. There is little evenness between the right side and the left side of the body. The arms and legs are stiff and have little charge. His gaze seems unfocused and distant. The main aliveness is deep in the torso and in the head. He seems to have little natural muscle tone. In somatic character reading, this posture translates into: holding together against fragmentation, and contraction toward the body core and into the head. The posture shows strong tension at the base of the skull, corresponding to the activation of the earliest startle and orienting reflexes.
Some character structures are described in similar ways in different systems but assigned to different developmental stages. Most notable is perhaps the hysteric, which Bioenergetics and Hakomi describe as a “genital” or “oedipal” structure. Bodynamics sees the hysteric as part of the schizoid or existence structure, a result of the “schizoid-hysteric split” first described by Lake in 1966. Boadella (1986) considered the schizoid versus the oedipal theory of the hysteric structure and pointed out that an infant who feels compelled to fling himself into contact for dear life is quite likely to expand his survival strategies with flirtatious and seductive behavior when he or she reaches the oedipal stage. The two explanations can then be understood as complementary, rather than mutually exclusive.
When deeply frightened, an infant will flail, scream, and “try to grab” his parent with his eyes and intensified gripping reflexes. If this feeling of threat and coping strategy is internalized as a representation of being in the world, the adult is likely to feel threatened by fairly small separations and upsets. He will respond with strong contact-hunger, emotion, and excitement in an attempt to get the interpersonal closeness that will help him feel less threatened. This is the inner landscape of the adult hysteric structure: “Saying good-bye is like dying” (Lake, 1966). The primary identification is with emotions, relationships, and the body. Often the person distrusts the mind and its silent machinations.
According to Lake, it is only when the threat becomes pervasive and seemingly unending, giving a sense of “no way out,” that the individual will withdraw into himself and into the state of the schizoid structure described above.
Bodynamics describes the adult hysteric (emotional existence) structure as “looking as if he has a small head,” and Hakomi (Ogden, 1985) describes the schizoid as having a long neck. Johnsen and Bodynamics find that the early gripping reflexes in the hands and feet as well as early neck reflexes are often also present. As in the schizoid, the body characteristics of this structure are fragmented, but more symmetrical. Joints are typically overly flexible rather than stiff. There are lots of facial animation, expressive body movements, and lots of emotion.
Several somatic systems warn that this structure can be incorrectly assessed as healthy in traditions that rely heavily on encounter, contact intensity, and emotional catharsis, all central elements of the defense pattern of the hysteric structure.
The “overactive” infant, described by Brodén (2000), has no direct counterpart in the developmental somatic character systems. Lake, however, describes the schizoid-hysteric condition as a split branch, in which a person “flips” between the two stress responses of sympathetic and parasympathetic override. Both the schizoid and the hysteric structures can have elements of the overactive pattern. The hysteric generally lives in a continuum that stretches from a sympathetically charged, survival-motivated socialization to a desperately or chaotically agitated sympathetic fight-or- flight arousal with sudden dissociated pockets. The schizoid generally lives in a continuum that begins in the dissociated parasympathetic state and may be overridden by the chaotically agitated sympathetic fight-or- flight state under extreme stress. If the person has more contact-seeking characteristics, he will generally be assessed as more hysteric, whereas the contact-avoidant individual will be assessed as more schizoid.
II. The First Year: The Maturation of the Limbic System; “Schemas of Being With”; and the Oral-Depressive and Oral-Paranoid Structures
In terms of neurological development, the first year is characterized by explosive neuronal growth. This growth is intimately shaped by the specific life conditions and interactions in the infant’s new social environment. The primitive brainstem structures are already functioning, and the mammalian vagal system will mature during the first several weeks. At around six weeks, the infant is capable of interactive facial and eye expressions, which makes mutual gaze interactions possible. The amygdala, a part of the limbic system that is already active at birth, gives the infant the capacity to have emotional experiences linked to external events. Although the amygdala is known for its function in aversive conditioning, this ability only matures some time after birth. This maturational difference permits early attachment, regardless of parental behavior (Schore, 1994). Until the capacity for aversive learning has matured, the infant will continue to turn toward an insufficient or abusive caregiver, but will respond with stress and fear while doing so (Sullivan et al., 2001).
The amygdala is central to forming emotional memories: Damasio (1994) and LeDoux (1989, 1996, 2002) point out that it receives input from many other brain structures. During the first year, the amygdala ripens to be able to process and coordinate sensory and kinesthetic information and emotive response (later in life, it also assesses information from higher cortical areas of the brain, allowing more considered responses).
The brain areas involved in the mirror-neuron network also mature during the first year. In the first two months of life, exact mirroring and simple rhythmic attunement are central to interaction. After two months, the empathic information from the mirror system allows the infant and caregiver to establish complex interactions (Trevarthen, 1993a, 1993b; Tronick and Weinberg, 1997), as the implicit mirroring allows a growing feeling of each other’s intentions and inner states (Keysers, 2011). In the process of developing intersubjectivity, sense of self, and belonging, play activities are enormously important. There is a specific brain network involving areas of the limbic brain (Panksepp and Biven, 2012), and play activities begin in the first few months of life with exciting coordinated psycho-motor interaction games with the caregiver, such as playful tickling and “I’m coming to get you!” Later, the child graduates to rough-and- tumble play with the caregiver, and later again to peer play and role-play. This has led Panksepp (Ibid.) to wonder why play activity, with its strong anxiety-and depression-reducing properties, is so underutilized in psychotherapy.
The orbitofrontal cortex undergoes rapid maturation from around eight to eighteen months (Schore, 1994), and is central to the ability to form attachments and relate in meaningful sequences. This part of the brain handles emotional evaluation. Positioned between the limbic system and the frontal cortex, it is central to the capacity for self-regulation of affect, and the regulation of the autonomic nervous system, while also forming the basis of cognitive assessments. The inner state of caregiving strongly activates the fronto-limbic cortex in the caregiver. In the infant, the orbitofrontal cortex is strongly involved in the internalization of love and safe caring.
A number of motor skills are central in the development of the infant during the first year. In the earliest months, the coordination of sucking and swallowing is established, as well as that of eyes, neck, and facial expression. These abilities are crucial to the infant’s contact with his mother and to his ability to follow her with his eyes. He is also exploring the rest of his visual world, and, as voluntary reaching, gripping, and handling overrides his inborn gripping reflex, he can reach for and handle the things he sees. Letting go is more difficult, and is learned between the fifth and twelfth month. Around six to eight months, after some intensive training sessions of simultaneously lifting arms, legs, and head while belly-down on the floor, the infant’s spine strengthens to the point that he can actually sit up straight. This heralds the beginning of rolling, scooting, and creeping, which quickly give way to crawling, standing, and walking with hand support as his legs begin to hold his weight and their coordination improves. He launches into exploring the world, his capacity to handle arousal grows, and his needs differentiate. The loving, regulating, and encouraging caregiver shapes the emotional tone of the sense of self that he develops during these processes.
Stern (1995, 1977/2002) has studied mother-infant interactions during these crucial months. His phrase “schemas of ways of being with” is a term for the internalization of early contact experiences. He describes the following interaction as typical of an infant with a passively depressed mother, not an agitated or anxious one—one who has become so after the infant has some experience of normal behavior and developed some schemas for it.
The infant attempts to engage and “reanimate” the mother, but is unsuccessful. He then responds with resonant affect and motor changes: his posture deflates, his positive feelings drop, and his face falls. Stern describes this as a “microdepression.” He makes the point that this microdepression is not only a response to lack of stimulation, but an imitative, resonant, or contagious process. At the neuroaffective level, this is an example of an emotional transmission through neurological mirroring, creating “limbic resonance.”
“The two phenomena—being with via identification and imitation, and the experience of depression—become linked in a single moment of subjective experience” (Stern, 1995, p. 101). When this happens repeatedly, the infant establishes a schema of being with Mother, a norm, in which he imitates more and loses self-agency, as well as positive affect and motor competency.
Stern then goes on to describe a condition he has investigated in adults: that once this schema is in place, the desire to be with someone will in itself trigger the microdepression. Stern repeatedly and decisively points out that the infant is not a telepath, and that he cannot know the mother’s fantasy world. What he can know is how she is responding to him. This he knows intimately and minutely in the delicate dance that they share. Stern here mentions the difficulty of having an observer correct a poorly attuned mother in this attunement process. Corrections make her self-conscious and awkward, and the dance is lost, with mother and child still struggling.
During the first six months of life, the infant is interested primarily in dyadic contact, and develops “schemas” for all his family members, as well as for the recurring events in his life and their variations. In the second half of the first year, the infant’s ability to handle excitement grows enormously. His grasp of his inner and outer world is becoming increasingly differentiated and complex. At around six months, his interest turns toward the object world, and the role of his mother changes from primary focus to one point in a triangle: the triangle of mother, infant, and the plaything or the other person currently under investigation; both this triangle and the differentiation require much greater flexibility and maturity from the mother. Her baby needs her to read and care for his differentiating needs and feelings correctly, to be in affective visual contact when needed, and to be both a safe companion and a delighted supporter of his exploration of the outer world.
In the “hierarchy of needs” for the growing child, Bioenergetics suggests that the issue in the first year of life is the right to have needs, to differentiate them, and to be loved as a separate being. The formative dynamic of the “oral” character structure is thought to be lack of early interpersonal nourishment and support or, less commonly, deprivation of physical nourishment. The mother is seen as either unavailable, weak, depressed, ill, or resentful of the differentiating needs of the child. As inchoate inner needs emerge and are not mirrored or responded to, the child collapses into a state of helplessness and resignation. This experience is internalized as a self-representation of being infinitely needy and unfulfilled in a world with no gratification available.
The early, depressed structure is often described as needy, compliant, dependent, overly verbal and helpless. He is seen as sucking others’ energy. The dynamic of “trying to get mother to react right” and the microdepression following failure is also described in the oral patterns. With pleasant invitation and compliance, the adult tries to get the desired closeness in his relationship to intimates or to a therapist. However, his attempts are colored with resignation, as if he “expects a no.” Sørensen (1996), chief psychologist of a Danish psychiatric ward, describes the early oral structure as always ready to engage, if there is a chance of contact (p. 188) and grateful to get what he can, but without the kinesthetic sense of self needed to discern the quality of the interaction, or whether it matches his needs. This is partly because he fails to recognize what he is getting while he gets it, and partly because his containment and object constancy is poor—he quickly loses the feeling of being full and satisfied.
Bioenergetics, Bodynamics, and Hakomi all describe similar postures in the oral stage. Both early and late “oral” character types have a collapsed “S”-shaped spine, sunken chest, head held forward, and weak legs with locked knees. This description of low energy and motor passivity corresponds well to Stern’s description of the infant in microdepression.
The flaccid belly protrudes like a “half-filled sack” (Lowen, 1958). The early oral structure is described as having a weak, longing gaze and soft, inviting lips, whereas the late oral structure is described as having a more aggressive, suspicious expression, and either pouting mouth or clenched jaws. The energy flow is described as weak in the whole body, especially in the arms and legs. The strongest and most contactful energy is in and around the mouth and eyes. These physical characteristics correspond to specific levels of neuromotor maturity. Before six months or so, the baby’s deep intrinsic spinal muscles and muscles of the torso cannot yet hold him upright in the sitting position for any length of time. The same muscle groups seem unable to hold the adult oral structure in a wholesome, erect standing or sitting posture. In the infant, the neck muscles and the eye-head coordination have matured in the first couple of months. Correspondingly, the adult in the oral structure uses his neck and head position to compensate for the weak postural capacity of the torso.
The dissatisfaction in the late oral structure is understood to correspond to the infant’s unhappiness with having his increasingly differentiated needs and feelings incorrectly “read” and responded to by the caregiver. A dissatisfaction of this rather sophisticated nature is generally predated by a better “match” or “reading” at the earlier, less complex stages of interaction. The adult late oral structure distrusts the authenticity or validity of what is given, and expects it to be withdrawn without notice. This thwarts his deep desire for closeness and exciting interaction. Hakomi (Weiss, 2003) states that this structure had enough determination and strength to erase totally the option of support, and instead rely on itself: “I will not expose myself to that yearning ever again and be in pain forever.”
Another effect of incorrect reading by the regulating caregiver is incorrect identification of one’s own needs and feelings. The infant develops schemata of “being with” through resonance and interactive response. Schemata based on incorrect mirroring will not satisfy him, nor will they sufficiently regulate or mature his affective state or his interactions.
In the adult interaction, the late oral structure has a set idea of what he needs and should have, complete with the frustration of not getting it right, based on his incorrect schema. This means that attempts to satisfy him usually fail partially or completely. He then either fumes silently, because he does not trust anything that is not spontaneously given, or he impatiently tries to “correct” the other until he gets exactly what he wants. In both these scenarios, sensitive two-way attunement and discovery of how to match the inner state with the “right next action” are lost. As in Stern’s corrections to the misattuned mothers, the dance is lost, he cannot find his way to it, and his attempts to find it push it further away.
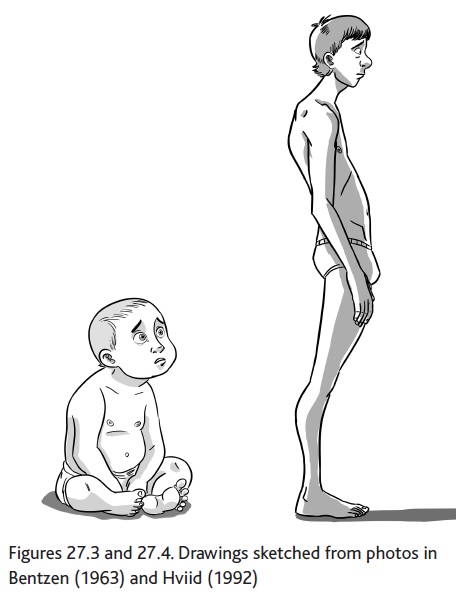
Oral Somatic Pattern
The oral structure is shaped by threat of abandonment. (Bioenergetics)
Formative age: birth through eighteen months (Bodynamics). Called the oral stage of development by most systems. This baby is sitting up (Figure 27.3), but his spine is not yet strong enough to hold him in the upright position. He collapses, and his head angles upward awkwardly to make eye contact. Except for the head position, this is also the posture of the motor collapse of the infant in “microdepression.” This early stage of somatic organization is thought to define the oral posture of the man (Figure 27.4).
His spine is collapsed, his head falls forward as he gazes longingly into the world, and his arms and legs are passive. In the standing position, spinal collapse forms an “S” curve, rather than the infant “C” curve. There is a general sense of low tone and little strength in the body, especially in the arms and chest. This posture is read in somatic character systems as “collapsed,” but holding on against abandonment.
III. Eight to Fifteen Months: Orbitofrontal Elation, Inner Representations, and the Psychopathic Structure
Toward the end of the first year, a great many powerful new cortical developments occur. From eight to fifteen months, the brain undergoes a massive pruning of synaptic connections, in which unused connective possibilities are culled. Such pruning occurs several times during childhood and is probably related to qualitative leaps in affective and cognitive organization.
At around nine months, the infant becomes able to manage much higher levels of pleasure and excitement, particularly in intense dyadic contact with the mother. From about ten months to thirteen and a half months, a strong heightening of positive affect and lowering of negative affect is observed (Schore, 1994, p. 132). Neurologically, this elation reflects the development of dopamine circuits from the limbic system and into the orbitofrontal cortex, which “comes online.” The orbitofrontal cortex is central to the linking of externally experienced events with internal states and feelings. The right lobe, related primarily to emotional processing, is larger and has much stronger connections into the limbic system than the left lobe does.
This right-brain maturation allows the toddler to form an inner schema of the different emotional expressions of his mother, linking them to his own inner sensory and emotional response. Also, he begins to have a sense of time, or temporal coherency. This allows him to form an experience-based representation and expectancy of future events, which he uses to guide his actions. In other words, the orbitofrontal cortex is the center of object constancy. However, the maturation of complete inner schemata seems to depend on the development of high levels of dopaminergic excitement in the relationship, and it may be disturbed both by insufficient arousal and by hyperarousal. Burton and Levy (1991; see Schore, 1994, p. 191) suggest that, with insufficient arousal, the toddler’s representations remain more primitive and piecemeal. Hyperarousal, on the other hand, is thought to lead to unmodulated rage responses. Gaensbauer and Mrazek (1981; see also Schore, 1994, p. 207) describe a mother teasing her infant from anger into a state of unmodulated rage.
In terms of psycho-motor organization, the infant becomes capable of independent locomotion at about ten months. He begins autonomous explorations of the world, crawling and toddling out into the environment, frequently returning to interact with, touch, or lean against the caregiver. Mahler described this stage as the practicing period, and the behavior is aptly called “psychological refueling” (Mahler, Pine, and Bergman, 1975). At this age, the beginning autonomy of the infant greatly expands the complexity of intrapsychic and interpersonal events, and the somatic character systems focus on somewhat different aspects of this complexity in their personality descriptions.
Bioenergetics describes the basic issue of psychopathic structure as the “right to be free” (from the manipulative needs of others), and the somatic tension pattern as “holding up against falling down.” In Hakomi, the psychopathic structure is linked to the long process of the child forming a self-image, and learning honesty in needs, weaknesses, intention, and feeling. In Bodynamics, the (activity directing autonomy) structure is organized around the toddler’s excitement with his impulses and ideas, and his insistence on following his own desires. Bodynamics sees the unmodulated excitement of practicing, and the late-practicing- age social and sexual exploration as the basis of this structure.35
The early practicing child needs help to modulate some very high states of excitement, and the mother may not be able to do this. Unregulated high arousal becomes disorganized. In the child, this becomes evident as the child’s involuntary excitation and entrainment keep him active—perhaps crawling or walking—until he is crying with fatigue, but still can’t stop himself.
One formative dynamic of the psychopathic structure is thought to be the relationship to a mother who is extremely manipulating. She induces the child to believe that he can manage by himself. She denies his helplessness or is afraid of it, and ignores his neediness and weakness, focusing only on his strengths. In this stage of basic reality testing and subsequent modification of inner schemata, she does not help him test reality, so he maintains grandiose and unrealistic images of himself and his abilities.
Another theory is that the mother is overly excited by the accomplishments of her child, and is overidentified with him. This means that, instead of being with a containing, sharing, and regulating mother, the child is met with an escalating excitement that overwhelms him, making him lose track of his own feelings and activity in the surge of maternal affect and contact. He then begins to avoid contact with the overstimulating mother, and, in the absence of her regulating contact, he forms a more partial schema of his inner states and emotions. Driven by the inner dopamine high, he dives into the sympathetic excitement and intense task-absorption of the practicing child, and denies the vegetative needs that would lead him back to the mother, about whom he is now ambivalent.
In the adult psychopathic structure, this excitation shows up as a constant and passionate drive onward to the next activity, with no time for reflection, completion, or digestion. He is perennially excited and enthusiastic about whatever he happens to be doing at the moment, and his enthusiasm is very catching. He is extremely resistant to negative feelings, and moves on to the next passion as soon as he gets bored, or develops unpleasant or ambivalent feelings with his activity. He immediately forgets or suppresses negative interactions and feeling states. He is extremely hard to “pin down” and correct. If this is attempted, he may respond with extreme rage. This structure corresponds to the high-arousal dopamine-activated hyperactivity seen in the practicing stage.
The psychopathic structure’s inner representation of self and world is that he has to do it himself—who else is there? He may help other people, but he doesn’t feel that he needs help—he doesn’t recognize feelings of inadequacy or neediness, because schemata for them are partial or missing. Underlying this is a fear of being engulfed by the mother.
The somatic holding pattern of the psychopathic structure is: tense legs, a tight pelvis, tends to walk on his toes, and lifts his whole body up by the shoulders. He has a magnetic gaze, and a very engaging manner. He is described as having his energy displaced upward, and tends toward motor and verbal activity.
The practicing-age infant walks on his forefoot. His falling reflexes in his arms and shoulders are just beginning to become active, and he uses his arms and shoulders to keep his balance as well as to handle objects and play with people. He is “up” in his own body, and is also fascinated with getting up on high things—climbing stairs, chairs, kitchen counters, or even refrigerators, to the horror of parents and caregivers. The social charisma, excitement, and varied “language babble” are also typical of the practicing stage.
Psychopathic Somatic Pattern
Formative age: eight months to two and a half years. (Bodynamics)
Hakomi states that the formative age is before four, while the child is developing its self-image in interaction with the image held by others. This early toddler is flooded with excitement (Figure 27.5). He is passionately focused outward, and is intensely engaged and engaging. He is walking, but his legs are not yet fully up to the task and he is using his shoulders, arms, and hands to keep his balance. His energy is going up in more ways than one. If his legs do not stabilize, he may become a toe-walker and have trouble developing normal walking and push-off.
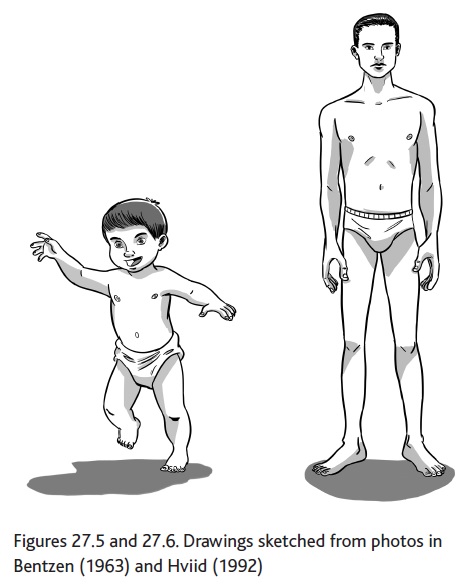
The somatic organization of the man in Figure 27.6 is similar to that of the young toddler. He has overdeveloped, square shoulders, a tight pelvis, and tight, thin legs. He is standing on the forefoot, with little or no weight on his heels. Although a drawing does not show it, he probably holds his balance with a lot of subtle movement. His gaze is magnetic and engaging. In a somatic reading, this posture would be interpreted as displaced upward and outward, probably to avoid the fear and ambivalence that this structure associates with a deeper sense of the kinesthetic self and with the supporting floor; the relationship to grounding is often considered a clue to the relationship to the mother, the first environment.
IV. The Second Year: Inhibitory Regulation and the Masochistic Structure
In the beginning of the second year, the intense pleasurable dynamic and interaction of the previous months changes radically. The earlier general state of pleasurable dopaminergic excitement is now followed by a period of anxious, depressed, shame-responsive hypothalamic-pituitary- adrenocortical (HPA) activity, starting between twelve and fourteen months. We are now at the end of the critical period for practicing, and the beginning of the rapprochement phase.
This development heralds the beginnings of the development of social inhibitory capacities in the child. Great importance is placed on the development of shame. This intense swing from a positive sympathetic to a stress-deflated parasympathetic state is thought to activate further development of the fronto-limbic structure (affect regulation) and the maturation of the orbitofrontal cortex (object constancy and emotional assessment). The fearfulness, depression, sensitivity, and separation anxiety described at this stage of child development fits the descriptions of the emerging adrenocortical function. This affective state is triggered by normal misregulations as well as shaming interactions.
Some authors speak of an actual shift from a nurturing to a socializing relationship. Tulkin and Kagan (1972) note that the interaction with the ten-month- old is 90 percent centered on love and positive interactions, and 5 percent is used to limit the child. At around fourteen months, the child is exploring up to six hours a day, and the percentages of limiting interactions rise dramatically. The mother of the eleven-to seventeen-month- old intervenes to stop her child from some activity about every nine minutes (Power and Chapiesky, 1986; see Schore, 1994, p. 200). This means a great many interactions in which the toddler creatively tries to find ways of doing what he wants, while the parents try to prevent him from doing it. Many authors describe shaming as being a primary way that caregivers regulate the actions of their toddlers. Schore states that the ensuing frustration (in the toddler, not the parent) and internal stress trigger the further maturation of the cortex.
Absent at twelve months, embarrassment and shame are first seen in the toddler at around fourteen months. A shame-inducing reunion scenario might go like the following: In his foray into the world, the toddler has found a lovely, squishy, sweet-tasting thing on the grass, which he is bringing back to his mother. He is very excited and anticipating the intense pleasure of her delight and sharing. Mother looks at him, disgust etched on her features, and shouts, “No! Bad! Dirty ice-cream!”
With this strong misattunement, the toddler is abruptly plunged from a state of pleasurable, high-dopaminergic, sympathetic excitement into a sudden, stress-filled, parasympathetic vagal activation. His excitement is sharply inhibited, his heart rate abruptly slows, his body and limbs lose tonus, his head hangs, his face loses tone, and he blushes. His legs may even give way. He feels lost, and his mother seems like an alien being to him. It is now vital that his mother act to regulate him out of this state of intense shame, because his immature nervous system does not yet know how to do this for himself. He will probably try to make contact with her to reestablish the lost regulatory flow and, with it, the good inner feelings. If all goes well, his mother will now reattune and stay in contact with him until he is “back on his feet” again. Through this kind of interaction, the toddler’s sense of object constancy deepens as he incorporates that conflict and painful misattunements can be healed.
In a later typical regulatory situation, the toddler is heading toward a nice muddy puddle, and his mother, some distance away, breaks off her conversation with a friend, tenses up, and frowns at him. Because he is strongly sensitized to her nonverbal responses, he picks up this signal, pauses, and changes direction. The injunction has now become part of a more modulated dialogue. The toddler is internalizing his mother’s rules, and the socialization process is moving ahead.
Around eighteen months, shame signals are becoming an internal guiding system (Greenspan, 1988). Moving toward a puddle, the child may stop, remember his mother’s frown, frown in imitation, struggle a while between desire and inhibition, and finally turn away.
Newer psychoanalytic theory (Schore, 1994) suggests that the socializing function of shaming and shame are at the very heart of the development of a sense of self. It describes the toddler as living in a dreamlike present until the shaming parent and his own emotional response jerk him into full wakefulness. In this context of early ego formation, it is interesting to note that many theoreticians speak of the shame process, with its abrupt plunge into the dissociative vagal activation, as being one of the most intensely kinesthetic feelings that we experience (Ibid.).
Pathological exchanges may occur in this vital process. Unregulated parental expressions of rage and contempt evoke intense and unrelieved shame and humiliation. Shame-humiliation dynamics have been found to consistently accompany child abuse (Kaufman, 1989; Lewis, 1992; see Schore, 1994, p. 207). If the stresses of the child’s life are too overwhelming, he may become stuck in a vagally dominated state of diminished movement and interest in the environment, and a general activation of the anxiety-deflation- shame state.
In the somatic character traditions, Bioenergetics focuses on the right to be self-directed and on the somatic tension pattern of holding in against humiliation and shame. Hakomi states that the innate issues of the formative stage of the masochistic structure are responsibility and freedom, and that the structure “clamps down and sticks to the ground.” These two systems often see the psychopathic and masochistic structures as complementary. In Bodynamics, the threatened right of the (self-sacrificing will) structure is to make choices and develop one’s will. The structure is strongly driven by shame, guilt, and overresponsibility.
Although there have been attempts to distinguish decisively between shame and guilt, current findings indicate that guilt is a later modification of the same neurological processes as shame. As such, guilt is usually more specific and localized, whereas shame is usually more global and pervasive. The formative age of the masochistic structure is traditionally the anal stage (in Bodynamics, two to four years). Because the affective processes of socialization and shaming, and the body postures related to it, emerge around fourteen months, it seems reasonable to set this as the beginning of the formative “window” of this structure.
The masochistic structure is thought to have the following formative dynamic: The primary caregiver overcontrols, nags, rages, or shames the child, and the child responds with shame and guilt. He collapses into anxiety and self-judgment, and draws back from asserting himself in relationships as well as in activities. Fearful of asserting himself, he also turns his anger inward.
The masochistic structure’s inner representation of self and world is that he is deficient. He is locked in a struggle to be good, and he fails abjectly. He feels that his failure is the cause of all kinds of calamities—his own accidents, his mother’s pain or illness, and nebulous unknowable catastrophes. His representations are much more complex than those described in earlier structures, because this structure spans a later and more diverse range of cognitive development. Because the ability to form object-representations has reached a level of beginning causal and temporal coherence, the masochistic structure can be immobilized by fear of the future as well as fear of the consequences of his actions. He is self-effacing and submissive, and afraid of choices and independent action. He takes on burdens and either fails or is driven by fear of failure. Hakomi and Bioenergetics sum up the central belief of this structure: “Submission is the price for intimacy.”
This description corresponds to an ongoing neurological dynamic of anxiety-worry (hypothalamic-pituitary- adrenal activation) and a constant level of inhibitory shame. Accordingly, the masochistic posture is based on a shame-or guilt-based collapse in the spine, and hunches inward like a shamed toddler. The butt is tucked under, and the shoulders are drawn protectively up and forward.
Another aspect of this structure is the sense of burdens. Beginning around the age of two, the child’s balance and gross motor control have now improved. He delights in carrying things around, and will test his limits by trying to carry objects that are too heavy for his body. He will also engage in “helping Mother,” practicing his entry into the world of responsibility. The masochistic structure typically takes on physical and emotional burdens and is ambivalent about them—wanting to do it right, but feeling overwhelmed and confused by the tasks he has accepted.
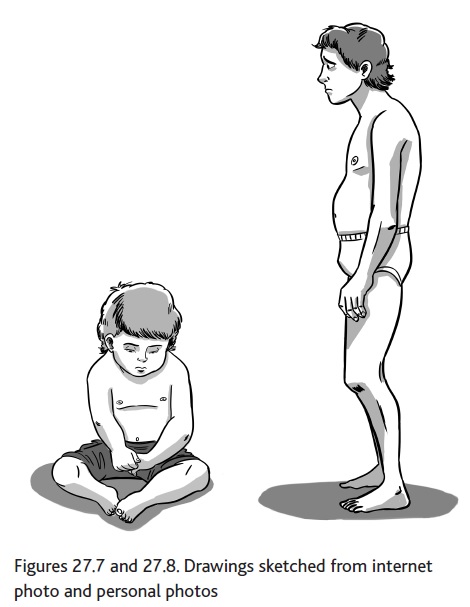
Masochistic Somatic Pattern
The masochistic structure is shaped by threat of humiliation. (Bioenergetics)
Formative age: two to four years (Bodynamics). Hakomi states that the formative age is when the child is becoming autonomous: learning to walk, move freely, and assert itself. This child is in the acute state of shame (Figure 27.7). He is hunching his shoulders, making an unhappy, shameful face, and squeezing down into himself in his seat on the floor. The head and neck are pulled into the torso. His arms and legs are flexed. Because motor control in his legs is still quite immature, he will find it hard to stand or walk in this state, but will tend to collapse to the floor or ground.
The adult is in a similar state of neuromotor organization (Figure 27.8). His back and shoulders are hunched forward, and he is “tucking his tail.” His facial expression is apologetic and suffering, and perhaps angry as well. His arms and legs are flexed, and he seems to be weighed down by an invisible yoke on his shoulders, and perhaps also invisible weights in his hands.
A somatic reading would describe him as weighed down by responsibility and tucking his tail in shame, while the solar plexus area, traditionally related to feelings of dignity and personal power, is collapsed.
Bioenergetics and Bodynamics both describe a later development of this structure: the sadistic (in Bodynamics: judgmental will) structure. It is described as having the same basic inner dilemma, but whereas the masochistic
structure submits to get intimacy, the sadistic structure rejects intimacy as well as submission and instead chooses self-assertion and loneliness. This structure takes a controlling, judgmental stance. Bodynamics (Bernhardt et al., 1996) describes that the child moves from self-correction to commenting on, correcting, punishing, and shaming the behavior of others. Bioenergetics describes the structure as being mixed with the later rigid structure and the issue of opening the heart. In Hakomi, these phenomena are seen as elements of the psychopathic structure. Bodynamics states that the child’s dilemma is that it is not allowed both personal empowerment and intimacy. The early, self-sacrificing structure gives up empowerment, and feels ashamed, dejected, and, under that, angry. The late, judgmental structure gives up intimacy, and is coldly and angrily controlling.
The posture of the sadistic structure is similar to that of the masochistic structure, but expresses anger rather than shame, and the spine behind the solar plexus is held aggressively straight instead of collapsing.
V. The Second Year: The Impact of Genital Sensory Maturation and Gonadal Steroids on Brain and Interaction, and the Rigid Structures
The most pervasive aspect of gender differentiation is linked to the level of sex hormones, which are very high at birth, and then slowly decrease through childhood, until they rise sharply again when the child approaches sexual maturity. From birth, high levels of sex hormones are circulating in the infant’s body. Impressive evidence has linked early gonadal steroids to establishment of sexual dimorphism in the maturing limbic system and cortex, including the orbitofrontal cortex (Schore, 1994). The neurological and psycho-social impact of these sex hormones in infancy seems to place the first beginnings of social gender identification at birth. Gender identification is critically dependent on social interactions. Nurturing contact raises the levels of gonadal steroids circulating in the infant’s bloodstream. The sex hormones then unlock genetic potential, and initiate sex-linked differentiation in the cerebral cortex and brain circuits. The sexual differences that develop during prenatal existence and during the first years become a permanent part of the brain. These include differences in the regulation of sexuality, aggression, and emotion as well as spatial coordination. This sexual dimorphism extends to the differentiation and use of the right and left hemispheres, and influences, among other things, the relationship between verbal and emotional processing.
In the middle of the second year, the child can correctly identify boys and girls. At around eighteen months, the gender process in the infant has matured to the point that both his brain and his sense of self have a definite and irreversible gender (Schore, 1994). Working models of maleness and femaleness, as well as personal identification, have already been internalized (Schore, 1994), and parents respond with pleasure to sex-typed play, rewarding boys for exploratory behavior and object play, and girls for quiet, social activities (Fagot, 1975; O’Brien and Huston, 1985).
The motor and sensory connections to the legs, pelvic floor, and genitals mature rapidly during the second year of life, and around the age of eighteen months the toddler becomes much more interested in touching and exhibiting his genitals (Kleeman, 1966, 1975). This development occurs when the shame response has been established for some months, and the two dynamics often become intimately connected (Nathanson, 1987). Parents frequently respond with embarrassment or shaming when the toddler fondles his genitals. According to Reich and Lowen, shame is a basic part of the regulation of the sexual drive.
At this time, the practicing period offsets, and, according to Schore, the imprinting process on the mother offsets too. The toddler is beginning to establish deeper relationships to other people besides the mother, and is developing his first experiences with triangular relationships. This process began with people and objects in the middle of the first year, but now he actively seeks other adult and child contacts, and experiments with them. With his parents, he begins to pull one close while pushing the other away. He may try to keep this triangular balance for minutes or days, but sooner or later he will try the opposite configuration, and “switch intimacies.” In this process, he seems motivated partly by a desire to test his power to direct the situation, but he also seems to be “feeling out” the different qualities of claiming an alliance with one parent while holding away the other. Ganging up with his father feels different from ganging up with his mother. Schore (1994, p. 267) also briefly mentions a theory of “father-imprinting” that is thought to onset at this time.
These behaviors, beginning in the middle of the second year, correspond to the dynamic described as “oedipal,” commonly held to belong to middle childhood. In light of the above research findings, it seems reasonable instead to set the beginning of the formative age of gender identification and interaction at birth, or at least at eighteen months, at the onset of irreversible gender sense, genital sensory maturation, and interpersonal triangular experimentation.
The somatic systems differ in their views of the posture and personality of the character structures of the oedipal, gender-differentiating period.36 Bioenergetics, Bodynamics, and Hakomi roughly agree only on the posture and personality dynamics of the rigid-phallic structure. For the other oedipal character structures, there is little agreement, as the three systems focus on different mixtures of oedipal structure with preexisting oral, psychopathic, masochistic, or schizoid-hysteric character traits. The reason for this general confusion might well be that the neuroaffective origins of schizoid-hysteric, oral, psychopathic, masochistic, and oedipal stages are closely knit and even have large developmental overlaps in time. The three systems focus on different clusters of postural and personal characteristics that emerge and intermingle during the first eighteen to twenty-four months, whereas the traditional psychodynamic view is that these patterns develop more sequentially during the first six years!
The rigid-phallic structure is identified with performance, both sexual and task-oriented. Hakomi and Bioenergetics describe it as industrious and overly focused. In Bodynamics, inspired by the works of Erik Erikson, gender issues have been separated from achievement issues, which are placed at Erikson’s (1950) “age of industry,” around preschool and school age. These later issues will not be described in this chapter.
Bodynamics notes that the key to the gender-differentiating (oedipal) stage is the quality of interaction and assigned identity: if parents define the child as sexual, whether good or bad, this is the identity he will internalize. If the interactions, and the child, are defined as sweet and loving (energy coming from the heart) and not sexual, whether good or bad, that is the identity that he will internalize.
The phallic structure has a lot of energy and excitement, more than any other character structure. He is organized around the internal experience of needing to be grown-up, or to achieve, or to perform. He is afraid of opening his heart to—another— rejection. He is afraid of opening himself, relaxing, and losing control, so despite his very high level of performance, he cannot seem to attain satisfaction and release. Bioenergetics and Hakomi describe both structures for both sexes, but Bioenergetics sees the rigid-phallic as more common in men, and the hysteric as more common in women, although this cultural pattern is changing. Bodynamics’ (seductive) position has a high charge in the pelvis and genitals, and a hurt, guarded closure in the chest and heart, corresponding to the Bioenergetic and Hakomi descriptions of the rigid-phallic structure.
In Hakomi, the formative belief of the person with a phallic structure is that he is not good enough to have a place in the adult world. Just “being” is not enough, and not good enough. One central interaction thought to lead to the phallic structure is that the father rejects the child or makes him feel inferior. The child struggles to “grow up fast” and attempts to take adult gender roles and responsibilities. Another dynamic is the parental requirement that the child be a “little man” or “little lady.” The love and acceptance of the parent depends on how well the child lives up to this demand.
The phallic structure has internalized the following representations of self and world. He feels fully alive and fully himself only when engaged in a task, or right after finishing it. He feels that he must achieve and strive to be the perfect man/woman/executive/doctor/dancer, etc. Only if he succeeds will others love and recognize him, or alternately: will he be worth loving and recognizing?
Rigid (Phallic) Somatic Pattern
The rigid structure is shaped by fear of surrender. (Bioenergetics)
Formative age: three to six years (Bodynamics). Hakomi states that it occurs when the child is old enough to be aware of sexual differences. (The children shown here are four to five years old, the age traditionally assigned to the oedipal stage.)
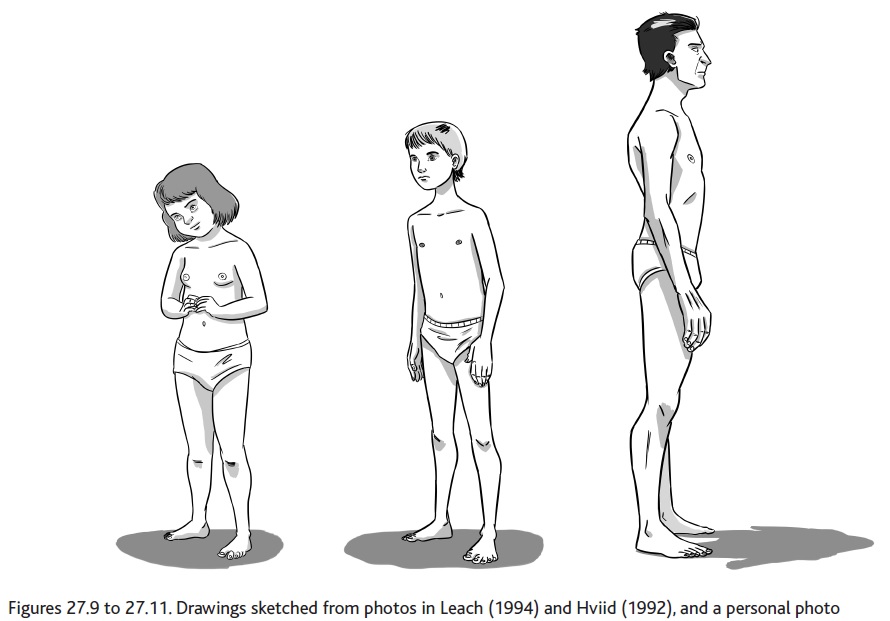
In her posture, this girl shows both openness and innocent flirtation (Figure 27.9). Her head is angled, and her facial expression is playfully inviting. Her shoulders and chest area, traditionally connected to heart feelings, is somewhat collapsed, and her pelvis and genital area show some congestion and fullness. Her chest seems smaller and more fragile. She combines the pelvic characteristics of the Bioenergetics mixed-rigid structures or Hakomi’s hysterical structure with some of the characteristics of the Bodynamics romantic structure.
The boy has the typical leggy and straight posture of middle childhood (Figure 27.10). His back is straight and arched, his legs are tense, straight, and muscular, and the general sense is of energy and presence. His shoulders and arms show a neuromuscular “readiness” to do something.
The man has a similar somatic organization (Figure 27.11). His posture is straight and confident, his spine is overarched, his legs are straight and tense, and his shoulders and arms are ready for action. His body is symmetrical, powerful, and controlled. His face shows tension. The whole posture has an upright tense quality.
In a somatic reading, this posture has a lot of “life energy,” but uses it to keep control, stay on top of things, and achieve, achieve, achieve. He is holding back against the fear of surrendering to softer feelings and to vulnerability.
Not surprisingly, the postural characteristics of both the phallic and hysteric structures epitomize some of the gender stereotypes of our culture. The phallic structure has a straight posture, with a shapely, tense chest and a tight, charged pelvis. His back is straight or arched, his legs are straight, and the general impression he gives is of a “good soldier” (Hakomi), a “toreador” (Bodynamics), or a “knight”—in either chain mail or plate armor (Bioenergetics).
Hakomi describes the oedipal-hysteric structure as expressive and clinging, like the schizoid-hysteric of Lake (1966) and Bodynamics. This structure is identified with his feelings, and is very sensitive and easily upset. He exaggerates emotions and is theatrical in his expression. He tends to have trouble focusing, is easily distracted or scattered, and is often inconsistent. Hakomi and Bioenergetics also state that he tends to use sexuality as a form of defense against deeper feelings and commitments. He may be promiscuous, or have his sexual activity with one person while he has his heart and deeper companionship (nonsexual) with another. He is often seductive or flirtatious.
Bodynamics’ romantic structure has overactivity or openness in the chest and heart, is wasp-waisted, avoids feelings and sensations from the genital area and the pelvis, and exaggerates ideals and loving feelings. The posture is similar to that of Bioenergetics’ hysteric structure.
Hakomi describes the body of the hysteric as being like a child’s upper body in a wide pelvis. The shoulders, arms, and chest are all underdeveloped and tense, and in the woman the breasts are often small. The abdomen and pelvis are soft, wide, and round. The posture is straight, and the head is held high.
The three systems describe similar formative dynamics for this structure. The parents reject the child’s sexuality, perhaps because they are afraid of their own sexual feelings for him. One commonly described dynamic is that one or both parents are contactful in the first years, but then withdraw and lose interest. The parents may also reject the child’s feelings and desire for loving intimacy, or deny the child’s growing individuality and personhood.
The hysteric structure has internalized the following sense of world and self. He feels that his love and his feelings are not enough or not good enough, or they are too much, and he is searching desperately for someone who will accept him “as he is,” while simultaneously withdrawing from the deeper involvement that would make his heart vulnerable to another wounding. Unlike the phallic structure, he feels his hurt and betrayal, and is identified with it. He therefore sees other people as being potentially wonderful and potentially betraying, as he struggles with his inner yearning and distrust.
The mixture of oedipal and preexisting oral or masochistic characters—the passive-feminine structure for men, and the masculine-aggressive structure for women—have the wide pelvis and narrow chest/shoulders of Hakomi’s hysteric and Bodynamics’ early psychopathic structure. If we accept that socially formed gender identity begins at birth, it seems likely that “mixed” structures would originally form together.
As earlier mentioned, the sex hormones underlying crucial gender differentiation are all active from birth, and are regulated by the caregiving interactions at the onset of the oral process. Genital sensitivity and genital interest mature in the late practicing period. In the actual life of the toddler, elements of caregiving are interwoven with socialization, excitement, sexuality, shame inhibition, gender learning, differentiation of object-relationships, and social interactions with more people and in more complex situations. The many different views of somatic oedipal character formation reflect this complexity.
These reflections on the oedipal character formation conclude this reflection on neuroaffective development and somatic character. I have focused on neuroaffective and psycho-motor development during the first wave of brain maturation from birth to two years old as a primary window for the formation of adult character. This view conflicts with traditional theories, wherein the masochistic and oedipal structures form largely after the second year. However, looking at neurological maturation and interpersonal interaction, it seems clear that the child has all the basic affective personality components of the traditional five stages of character in place by the end of the second year. In the next section, I have some concluding thoughts about formative character dynamics outside the first wave of brain development and outside the scope of this chapter.
Other Perspectives on Character Development
Clearly, the whole personality is not developed by age two! The structures described above deepen and differentiate through middle childhood and the teenage years as new cortical, psychological, and somatic competencies mature (Giedd et al., 1999; Giedd, 2002; Shonkoff and Phillips, 2000) and as peer relationships become an important factor in character development (Shonkoff and Phillips, 2000; Cummins, 2006). Beginning around the age of two, a left-hemisphere verbal identity forms along with the development of language and the refinement of mentalizing capacity (Allen, Fonagy, and Bateman, 2008; Hart, 2011), which is the ability to empathically reflect on the feelings and actions of oneself and others, and is closely linked to stress resilience. Curiously, the differences between verbal and nonverbal identity formation have generated little interest in the field of character theory, whether traditional or somatic. The vast impact of peers and group identification processes around the early school age have been considered characterologically only by Erik Erikson (1950) and Bodynamics; and neither contemporary research findings on neurological changes occurring in prepuberty and puberty (Robinson, 2009; Giedd, 2002; Giedd et al., 1999) or the considerable body of child and adult studies on social-dominance motivation (Cummins, 2006; Dunbar, 1998; de Waal, 2006; Hart and Bentzen, 2012) is assimilated in psychodynamic personality theory.
Finally, there is the important issue of correlating somatic character to validated psychological personality tests. To my knowledge, two attempts have been made in the last decade to do this. Fehr (2006) describes strong correlations between the Bioenergetic structures and the generally accepted “big five personality traits”: openness to experience, conscientiousness, extraversion, agreeableness, and neuroticism. Glazer and Friedman (2009) report satisfactory correlations between different raters of Bioenergetic character, but low reliability when compared to traditional personality measures. Hopefully, this chapter opens the way for fresh studies of somatic character.
33Editors’ Note: This chapter is one of the first comprehensive attempts to tie recent findings from neuroaffective and neuromotor child development research into Body Psychotherapy, informed by Developmental Psychology, as developed foremost by Reich and Lowen. Bentzen illustrates how “dysregulation” in early developmental phases may affect the ensuing maturational process. She also relates the neuropsychology of child development to structures of somatic formation and to a theory on behavioral patterns that was conceptualized within the framework of Body Psychotherapeutic characterology.
34Although these structures obviously exist in both genders, only the male pronouns are used in this chapter, for simplicity of language: “he” instead of “he or she” or “s/he,” “his” instead of “his or her,” etc.
35Bodynamics also describes a collapsed psychopathic (activity avoiding autonomy) structure, corresponding to insufficient dopaminergic excitation in the practicing infant. The adult is described as having a wide pelvis and narrow, collapsed chest. Hakomi assigns a similar body type to the oedipal-hysteric structure, and Bioenergetics to the masculine-aggressive and passive-feminine rigid structures. Both the overlap in formative stages and the similar interaction dynamics of having excitement and charge denied or rejected may contribute to the difference in assignment of this posture and body type.
36Because the core issue of the rigid character structure is gender identification, and because family structures and gender roles are culturally set, different formative dynamics must be expected in different cultures. These character descriptions have been developed in the North American and northern European cultures, and may only be fully valid there.
References
Aitken, K. J., & Trevarthen, C. (1997). Self-other organization in human psychological development. Development and Psychopathology, 9, 651–675.
Allen, J. G., Fonagy, P., & Bateman, A. W. (2008). Mentalizing in clinical practice. Washington, DC: American Psychiatric Publishing.
Beebe, B., & Lachmann, F. M. (2002). Infant research and adult treatment: Co-constructing interactions. Hillsdale, NJ: Analytic Press.
Bentzen, B. S. (1963). Børnemotorik [Children’s motor skills]. Copenhagen: Gyldendals pædagogiske bibliotek.
Bentzen, M., Jarlnaes, E., & Levine, P. (2004). The body self in psychotherapy: A psychomotoric approach to Developmental Psychology. In I. MacNaughton (Ed.), Body, breath and consciousness. Berkeley, CA: North Atlantic Books.
Bernhardt, P., Bentzen, M., & Isaacs, J. (1996). Waking the body ego II. Energy & Character, 27(1), 38–50.
Boadella, D. (1986). Maps of character. Weymouth, Dorset, UK: Abbotsbury Publications.
Brodén, M. (2000). Mor og barn i ingenmandsland [Mother and child in no-man’s- land]. Copenhagen: Hans Reitzels.
Burton, L. A., & Levy, J. (1991). Effects of processing speed on cerebral asymmetry for left-and right-oriented faces. Brain and Cognition, 15, 95–105.
Chess, S., & Thomas, A. (1996). Temperament. New York: Routledge.
Cuhna, F., & Heckman, J. J. (2010). Investing in our young people. In A. J. Reynolds, A. Rolnick, M. M. Englund, & J. Temple (Eds.), Cost-effective early childhood programs in the first decade: A human capital integration (pp. 381–414). New York: Cambridge University Press.
Cummins, D. (2006). Dominance, status, and social hierarchies. In D. M. Buss (Ed.), The handbook of Evolutionary Psychology (pp. 676–697). Hoboken, NJ: Wiley.
Damasio, A. (1994). Descartes’ error: Emotion, reason and the human brain. New York: Grosset, Putnam.
de Waal, F. (2006). Our inner ape. New York: Riverhead Trade.
Dunbar, R. (1998). The social brain hypothesis. Evolutionary Anthropology: Issues, News, and Reviews, 6(5), 178–190.
Erikson, E. H. (1950/1993). Childhood and society. New York: W. W. Norton.
Fagot, B. I. (1975). Sex differences in toddlers’ behavior and parental reaction. Developmental Psychology, 10, 554–558.
Fehr, T. (2006). Multidimensional Bioenergetic Personality Analysis: A statistical approach. European Journal of Bioenergetic Analysis and Psychotherapy.
Gaensbauer, T. J., & Mrazek, D. (1981). Differences in the patterning of affective expressions in infants. Journal of the American Academy of Child Psychiatry, 20, 673–691.
Gallese, V. (2001). “Shared manifold” hypothesis: From mirror neurons to empathy. Journal of Consciousness Studies, 8(5–7), 33–50.
Gallese, V., Fadiga, L., Fogassi, L., & Rizzolatti, G. (1996). Action recognition in the premotor cortex. Brain, 119(2), 593–609.
Gallese, V., & Goldman, A. (1998). Mirror neurons and the simulation theory of mindreading. Trends in Cognitive Sciences, 2(12), 493–501.
Gerhardt, S. (2004). Why love matters: How affection shapes a baby’s brain. New York: Brunner-Routledge.
Giedd, J. N. (2002). Inside the teenage brain. Interview. Frontline.
Giedd, J. N., et al. (1999). Brain development during childhood and adolescence: A longitudinal study. Nature Neuroscience, 2(10), 861–863.
Glazer, R., & Friedman, H. (2009). The construct validity of the Bio-energetic character typology: A multi-method investigation of a humanistic approach to personality. Humanistic Psychologist, 27(1), 24–48.
Greenspan, S. I. (1988). The development of the ego: Insights from clinical work with infants and children. Journal of the American Psychoanalytical Association, 36(suppl.), 3–55.
Hart, S. (2011). The impact of attachment. New York: W. W. Norton. Trans. from Danish (2006). Betydningen af Samhørighed [The importance of cohesion]. Copenhagen: Reitzels.
Hart, S., & Bentzen, M. (2012). Jegets fundament: den neuroaffektive udviklings første vækstbølge og de neuroaffektive kompasser [The foundation of the ego: The first wave of neuroaffective development and the neuroaffective compasses]. In S. Hart (Ed.), Neuroaffektiv psykoterapi med voksne [Neuroaffective Psychotherapy with adults]. Copenhagen: Hans Reitzels.
Hogeveen, J., Inzlicht, M., & Obhi, S. S. (2014). Power changes how the brain responds to others. Journal of Experimental Psychology, 143, 755–762.
Hviid, T. (1992). Kroppens Fortællinger I Billeder [Body stories in photos]. Aarhus, Denmark: Modtryk.
Ingen-Housz, M. (2003). Personal communication.
Johnsen, L. (1976). En nøgle til livsglædens skjulte kilde [A key to happiness’ hidden source]. Copenhagen: Borgen. Danish ed. of Johnsen, L. (1981). Integrated respiration theory/therapy: Birth and rebirth in the fullness of time. Tulsa, OK: Private publication.
Kagan, J., Snidman, N., Kahn, V., & Towsley, S. (2007). The preservation of two infant temperaments into adolescence. Monographs of the Society for Research in Child Development, 72(2, Serial No. 287), vii.
Kaufman, G. (1989). The psychology of shame. New York: Springer.
Keysers, C. (2011). The empathic brain. Groningen, Netherlands: Social Brain Press.
Kleeman, J. A. (1966). Genital self-discovery during a boy’s second year. Psychoanalytic Study of the Child, 21, 358–392.
Kleeman, J. A. (1975). Genital self-stimulation in infant and toddler girls. In I. Marcus & J. Franin (Eds.), Masturbation (pp. 77–106). New York: International Universities Press.
Lake, F. (1966). Clinical theology. London: Darton, Longman & Todd.
Leach, P. (1994). Your baby and child. New York: Alfred A. Knopf.
LeDoux, J. E. (1989). Cognitive-emotional interactions in the brain. Cognition and Emotion, 3, 267–289.
LeDoux, J. E. (1996). The emotional brain: The mysterious underpinnings of emotional life. New York: Simon & Schuster.
LeDoux, J. E. (2002). Synaptic self: How our brains become who we are. New York: Viking Penguin. Lewis, M. (1992). Shame: The exposed self. New York: Free Press.
Lowen, A. (1958). The language of the body. New York: Collier Books.
MacIntyre, J., & Mullins, R. (1976). A “new look” at character: The Bioenergetic Training Manual for the first year in Bioenergetic Analysis, ed. and self-published by Michael J. Maley.
Mahler, M., Pine, F., & Bergman, A. (1975). The psychological birth of the human infant. New York: Basic Books.
Marcher, L., & Fich, S. (2010). Body encyclopedia: A guide to the psychological functions of the muscular system. Berkeley, CA: North Atlantic Books.
Nathanson, D. L. (1987). A timetable for shame. In D. L. Nathanson (Ed.), The many faces of shame (pp. 1–63). New York: Guilford Press. O’Brien, M., & Huston, A. C. (1985). Development of sex-typed play behavior in toddlers. Developmental Psychology, 21, 866–871. Ogden, P. (1985). The chart. In R. Kurtz (Ed.), Hakomi Therapy. Boulder, CO: Hakomi Institute. Panksepp, J., & Biven, L. (2012). The archaeology of mind: Neuroevolutionary origins of human emotions. New York: W. W. Norton. Perry, B. (2002). Childhood experience and the expression of genetic potential: What childhood neglect tells us about nature and nurture. Brain and Mind, 3(1), 79–100. Perry, B. D., Pollard, R. A., Blakley, T. L., Baker, W. L., & Vigilante, D. (1995). Childhood trauma, the neurobiology of adaptation, and “use-dependent” development of the brain: How “states” become “traits.” Infant Mental Health Journal, 16(4), 271–291. Perry, B. D., & Slavavitz, M. (2007). The boy who was raised as a dog: And other stories from a child psychiatrist’s notebook: What traumatized children can teach us about loss, love and healing. New York: Basic Books. Porges, S. W. (1997). Emotion: An evolutionary by-product of the neural regulation of the autonomic nervous system. Annals of the New York Academy of Sciences, 807, 62–77. Power, T. G., & Chapiesky, M. L. (1986). Childrearing and impulse control in toddlers: A naturalistic investigation. Developmental Psychology, 22, 271–275. Reich, W. (1949/1971). Character Analysis. Rangeley, ME: Orgone Institute Press; New York: Farrar, Straus & Giroux. Ridley, M. (2003). Nature via nurture: Genes, experience, and what makes us human. New York: HarperCollins. Robinson, R. (2009). From child to young adult, the brain changes its connections. PLoS Biology, 7(7). Rutter, M. (2006). Genes and behavior: Nature-nurture interplay explained. Oxford, UK: Blackwell. Sander, L. (1977). Regulation of exchange in the infant-caretaker system and some aspects of the context-content relationship. In M. Lewis & L. Rosenblum (Eds.), Interaction, conversation and the development of language. New York: Wiley. Sander, L. (1983). Polarity, paradox and the organizing process in development. In J. D. Call, E. Galenson, & R. L. Tyson (Eds.), Frontiers of Infant Psychiatry (Vol. 1). New York: Basic Books. Sander, L. (1987). Awareness of inner experience: A systems perspective on self-regulatory process in early development. Child Abuse and Neglect, 11(3), 339–346. Sander, L. (1988). Event structure of regulation in the neonate-caregiver system as a biological background for early organization of psychic structure. In A. Goldberg (Ed.), Frontiers in Self Psychology (pp. 3–27). Hillsdale, NJ: Lawrence Erlbaum. Schore, A. (1994). Affect regulation and the origin of the self: The neurobiology of emotional development. Hillsdale, NJ: Lawrence Erlbaum. Shonkoff, J. P., & Phillips, D. (Eds.). (2000). From neurons to neighborhoods: The science of early childhood development. Washington, DC: National Academies Press. Sørensen, L. (1996). Særpræg, Særhed, Sygdom [Eccentricities, peculiarities, symptoms]. Copenhagen: Hans Reitzels. Stern, D. N. (1995). The motherhood constellation. London: Karnac Books. Stern, D. N. (1977/2002). The first relationship. Cambridge, MA: Harvard University Press. Stern, D. N. (2004). The present moment in psychotherapy and everyday life. New York: W. W. Norton. Sullivan, R. M., Landers, M., Yeaman, B., & Wilson, D. A. (2001). Neurophysiology: Good memories of bad events in infancy. Nature, 407, 38–39 (quoted by R. Adolphs, The neurobiology of social cognition. Current Opinion in Neurobiology, 2001(11), 231–239). Tabery, J., & Griffiths, P. E. (2010). Historical and philosophical perspectives on behavioral genetics and developmental science. In K. T. Hood, C. T. Halpern, G. Greenberg, & R. M. Lerner (Eds.), Handbook of developmental science, behavior, and genetics (pp. 41–60). New York: Wiley-Blackwell. Thelen, E., & Smith, L. (1994). A dynamic systems approach to the development of cognition and action. Cambridge, MA: MIT Press. Trevarthen, C. (1979). Communication and cooperation in early infancy: A description of primary intersubjectivity. In M. Bullowa (Ed.), Before speech: The beginning of interpersonal communication. Cambridge, UK: Cambridge University Press. Trevarthen, C. (1990). Growth and education of the hemispheres. In C. Trevarthen (Ed.), Brain circuits and functions of the mind (pp. 334–363). Cambridge, UK: Cambridge University Press. Trevarthen, C. (1993a). The function of emotions in early infant communication and development. In J. Nadel & L. Camaioni (Eds.), New perspectives in early communicative development. London: Routledge. Trevarthen, C. (1993b). The self born in intersubjectivity: The psychology of an infant communicating. In U. Neisser (Ed.), The perceived self: Ecological and interpersonal sources of self knowledge (pp. 121–173). New York: Cambridge University Press. Tronick, E., & Gianino, A. (1986). Interactive mismatch and repair: Challenges to the coping infant. Zero to three: Bulletin of the National Center for Clinical Infant Programs, 5, 1–6. Tronick, E. Z., & Weinberg, K. (1997). Depressed mothers and infants: The failure to form dyadic states of consciousness. In L. Murray & P. Cooper (Eds.), Post-partum depression and child development. New York: Guilford Press. Tulkin, S. R., & Kagan, J. (1972). Mother-infant interaction in the first year of life. Child Development, 43, 31–42. Weiss, H. (2003). Personal communication.
Acknowledgment: Marianne Ingen-Housz, international trainer in Bioenergetic Analysis, kindly corrected my statements about Bioenergetic Analysis in this chapter. Any other mistakes are all mine.
Selection by Marianne Bentzen, anthologized in The Handbook of Body Psychotherapy and Somatic Psychology, edited by Gustl Marlock and Halko Weiss with Courtenay Young and Michael Soth, published by North Atlantic Books, copyright © 2015 by Gustl Marlock, Halko Weiss, Courtenay Young, and Michael Soth, Reprinted by permission of North Atlantic Books.